5. GROWING UP WITH A RARE DISEASE
Maura Foresti
In the previous chapter we discussed how challenging the experience of learning to be carriers of a rare disease is. Even when it is possible to process this news, and integrate it into one’s own world of thoughts and planning, having a rare disease – which, for certain genetic conditions, brings elements of human rarity into one’s life as a whole – is a very strong experience that does not remain confined in the body, but which can seriously impact the quality of life of the carrier and their family members, with important reverberations also on the life contexts of the subject and on an entire community that wants to take care of the health of its members. For this reason, the cure of rare diseases requires, over time, various appropriate medical, psychological and social interventions in order to contain their psychopathogenic potential (Rebecchi 2018). However, like many painful experiences in human life, rare disease also contains positive potential.
In this chapter, we will first try to describe the main areas of life that can be affected by a rare childhood-onset disease and possible treatment interventions; we then discuss the potential value of rare diseases for a human community.
5.1. The effects on the foundational relation of human mental development
This point has already been covered in part in the previous chapter (see 4.1. Prenatal Diagnosis, Chapter 4). Here it is important to add that a newborn child carrying a rare disease may not have the synchronic capacity, typical of a healthy newborn, to enter into the early relationship with the caregivers; it could also have adults who are much more anxious, when not pained and injured, and therefore have difficulty playing the role of partner in the foundational relationship of human development. In other words, this is a very disadvantageous situation, in terms of the attachment relationship as well (Bowlby 1958). Often, in this phase, couples report the painful experience of desperate solitude, of uncertainty about the future of the child, of wandering among specialists without a guide, of a growing feeling of anxiety and inadequacy towards a “difficult” or distressed child, in any case rare or different, for which nobody knows how to intervene. In this phase it is necessary to provide for an early and competent psychological intervention that monitors the relationship and attachment, which can indicate to the parents the skills of the child beyond the impairment, offering them alternative ways to synchronize with their rare newborn, and that can coordinate useful or necessary rehabilitation interventions: physiotherapy, speech therapy, psychotherapy or other specific interventions. To avoid these chilling experiences, careful coordination is needed between hospital care and territorial assistance, between the specialized centre for the rare condition, the paediatrician of free choice and the neuropsychiatry service of the territory of residence, and sometimes social services and institutions or schools. In other words, a network, a community must be present to take charge of the child and his or her parents. From the scientific point of view, however, it is necessary that the appropriate guidelines for each rare disease are prepared as soon as possible from the point of view of the knowledge achieved.
5.2. Psychological consequences of early hospitalization
Sometimes rare diseases can involve surgery or long hospitalizations in the paediatric age. In general, in the case of prolonged hospitalizations at the early stages of life, special attention is needed to try to contain the harmful effects both on the development of the child and on the early relationship.
Early and/or prolonged experiences of hospitalization, especially if surgical, in fact risk the sense of continuity and security as well as the basic trust necessary for building one’s identity. The limitation of the development of autonomy, linked to the reduced possibility of movement, the alteration of daily rhythms, the lack of usual social and family relationships, and the lack of positive stimuli, could further slow down the child’s psychomotor development (Robertson 1958). Psychological intervention at this stage will be mainly aimed at supporting parents, observing the attachment process and emotional development of the child, and offering timely interventions to support these fundamental processes despite hospitalization (Sarajarvi et al. 2006).
5.3. Communication needs for individuals with rare diseases
The strategies used by each child to cope with the same disease are different and depend on various factors: the child’s temperament and personality, the stage of development, whether there is a need for surgery, hospitalization, or therapies, the different past experiences, the family and social environment in which it is embedded, the type of disease, and the circumstances and life changes imposed by the disease itself. Because of this complexity, care interventions should be tailor-made for each child and his or her family.
From the early days of life, a child is a subject centre of will and sensations, inserted in a relationship of very close dependence on adults. Because of this duplicity of the infantile condition, it is important for attention to be directed to multiple aspects: both towards the family and caregivers as well as towards the child and his/her living environment. At all times of the treatment the operators must cultivate an attitude that aims to make the child, even when very small, aware of their reactions to the disease, and also of the reactions of their reference adults (parents’ fear, pain and sadness can be misunderstood by the child as a negativity that disappoints loved ones); furthermore, when the child is placed in school settings, it is important to help them understand the possible reactions of their companions (for example, some children may, even if in many cases erroneously, fear getting sick by attending a sick child) and help parents communicate effectively with the teaching staff to better welcome the child and their reflections of the hospitalization experience when re-entering the school context (some children tell the experiences of hospitalization to adults and classmates, or express them through games that may also have an aggressive background, creating strong emotions in their peers, which it is good for adults to know how to mediate and welcome).
After seven years of age, cognitive development gradually allows the child to understand diseases and therapies; therefore it is necessary during the medical examinations to share with the child the main information and awareness aspects in order to enable the child to understand and begin to manage his or her condition independently; it is, in fact, potentially very harmful for a small human being’s sense of self and identity to hear adults talk about them without being helped to understand what is said about them. Thus when parents ask to hide some aspects of the disease from their children, it is not good to contradict them, but it is necessary at least to offer them psychological advice that can help them reflect on the meaning and possible consequences of their choice. The quantity and quality of the information transmitted to the patient and family (diagnosis, prognosis, treatment) and the ways in which it is transmitted are fundamental, since they play a crucial role in the process of acceptance and adaptation to chronic disease.
5.4. The impact on caregivers
Even those who, professionally, take care of people with rare diseases find themselves in daily contact with strong requests for support and emotional help that can make them feel submerged and helpless, which creates a high risk of burnout: for this reason it is it is necessary to offer information and support to the staff as well. To avoid feelings of helplessness in carers, in addition to good psychological support, a good care network is necessary which the operator can feel part of. In this regard, the patient associations present in the area are essential, and in synergy with the carers can play a fundamental role for both patients and operators.
5.5. Family dynamics, from parents to siblings
The experience of a child sick with a rare disease has a profound impact on family dynamics. When a couple is expecting a child, it can be the fruit of different choices, or even be experienced as imposed by fate, but it always represents, in the human symbolic imagination, the fruit of the union of the parents. For this reason, the fact that a child is sick, or a carrier of a rare genetic condition, is full of meaning with a negative potential for the parents. It can be thought that the disease is a kind of punishment: parents often confess strong and frequent guilt feelings in these life stories. Parents can also experience illness as a great injustice and become overwhelmed with powerful feelings of envy, or inferiority, towards those couples who have given birth to healthy children; one may think that they their union was unfortunate, and that this disease is the confirmation or revelation of one’s defective nature. Moreover, if an unborn child is normally a source of joyful anticipation for a future full of promise, a sick child becomes an anguished potential of a future of disability, lack of autonomy, limitations imposed on the child and their parents, as well as a lifelong commitment for parents to bear along with a formidable source of anguish about the time that parents call “after us”. And this is how that experience of becoming parents, which in itself represents a challenge for the couple, becomes a test full of dangers when a child is born with a rare disease. It is not easy, in fact, to challenge the sense of pathological guilt, the feeling of generative failure and this looming sense of “after us”. In this phase, professional and specialist help is necessary in most cases. The Italian National Institute of Statistics, ISTAT, reported that the incidence of minor relationship problems or even the breakdown of the relationship is much greater in the case of the birth of a child suffering from a rare disease.
The presence in a family of a child with a rare disease, which necessarily requires a great deal of parental commitment and which worries them differently than a so-called “healthy” child, has a powerful impact on fraternal dynamics. Healthy siblings often have an incidence of psychopathological and conduct disorders much higher than the normal population. It is frequently a way to attract attention, the communication of a discomfort related to feeling healthy next to a sick sibling and, therefore, a feeling of guilt compared to a sibling for whom there are intense feelings of jealousy for the attentions that the sibling receives from their parents, even if it is considered more unfortunate; it is the communication of a guilt-related discomfort over the aggressive feelings that having a sick sibling can generate. These are some of the most complex and powerful psychological dynamics. This unease of the so-called “healthy” siblings, if caught early and treated by competent professionals, can be resolved; in contrast, if ignored, it can degenerate throughout life even in serious psychopathologies. A psychological intervention to support these families should always provide for a careful observation of family dynamics, supporting parents in explaining and reading the complex emotional intertwining of their children’s sibling relationships.
5.6. The transition to the adult therapeutic world
In light of what has been said so far, it is useful to mention another complex aspect of the care of the rare sick child: the transition from care centres dedicated to children to adult services. It is clear from the above that the care of a rare sick child requires specialist centres with periodic follow-up and staff capable of becoming reference figures for patients and their families. Here the transition to adult care services is a crucial moment in the life of a rare disease patient; for this reason it should not be a mechanical transfer from childhood to adult services, but a carefully planned process, aimed at responding to the medical-assistance, psychosocial, educational and vocational needs of adolescents and young adults with chronic conditions (Wright et al. 2018). For patients, transitioning to adult services means, in fact, enduring a new separation, interrupting another significant relationship, which is a relationship of care and also deeply emotional, to start a new unknown. For this reason, getting to know the new staff and the functioning of the adult services, and being aware of a collaboration between the two services, can help increase the sense of personal security during the transition phase. In order to plan the transition, it is useful to introduce this concept in advance to patients, right from adolescence, and to make contact with the adult team before the patient moves to the new centre, avoiding implementing it in times of particular patient stress.
5.7. Autonomy and extra-family life: from school to work placement
Finally, the issue of autonomy and relationships outside the family environment with the broader world is very important. Rare diseases differ greatly from one another in the impact on the life of the carrier. Some situations prevent one from reaching basic autonomies such as dressing and eating, and impact cognitive skills in various ways; others, on the other hand, only affect physical autonomies, or only cognitive skills. It is often difficult to predict at an early age the degree of impairment that will accompany a condition. It is a matter of following the subject and his or her parents in trying to develop the potential of mutual autonomy to the maximum. This requires exploring with parents their assessments, which could sometimes prove limiting for the child in achieving some possible autonomies, or which in other cases could lead to highly conflicting relationship dynamics; to avoid this it is necessary to support parents in finding solutions that can at least alleviate the burden associated with the child’s lack of autonomy.
Another major theme is, in fact, that of relationships outside the family: the literature indicates that a rare disease patient risks a more withdrawn and modest social life. This is variously due to the different conditions the patient might have, the objective limitations, the prejudices spread in society and, finally, also to feelings of dysthymia of the bearer subject, which can also lead to dysfunctional ways of relating to others. This area of the life of a rare disease patient can frequently require the intervention of specialists to support their good social, scholastic and working integration. It would be extremely important to immediately support a good relationship with peers. The inclusion in school and in the world of work are fundamental stages in the development of every human being and, in the case of a rare disease, the involvement of the school requires specific attention that varies from condition to condition. We have no way here to address this issue with the importance it deserves. The same could be said about job placement.
However, it is important to highlight here how the social inclusion of a rare patient derives, fundamentally, from the ideas that a community has about rare disease and disabilities in general (Zani, Cicognani 2000). Here is our brief reflection on the positive potential of rare diseases in a human society. The degree of civilization of a human culture is assessed by historians on the basis of several parameters, including the care of their sick. A society that pursues a value of perfection and success with too much absolutism risks falling into the violence that characterizes the myths of racial perfection, which have been seen in human history on several occasions. The encounter with the disease, with the fragility of human biology, on the other hand, allows us to recognize the limits of our nature and to recover the values of mutual care and respect for human value, regardless of any other possible consideration, thus inviting us to cultivate the values of collaboration and the virtues of prudence and reflexivity, which our time is increasingly confining in favour of the search for adrenaline-fueled experiences and competitiveness (Mancuso, Boncinelli 2008).
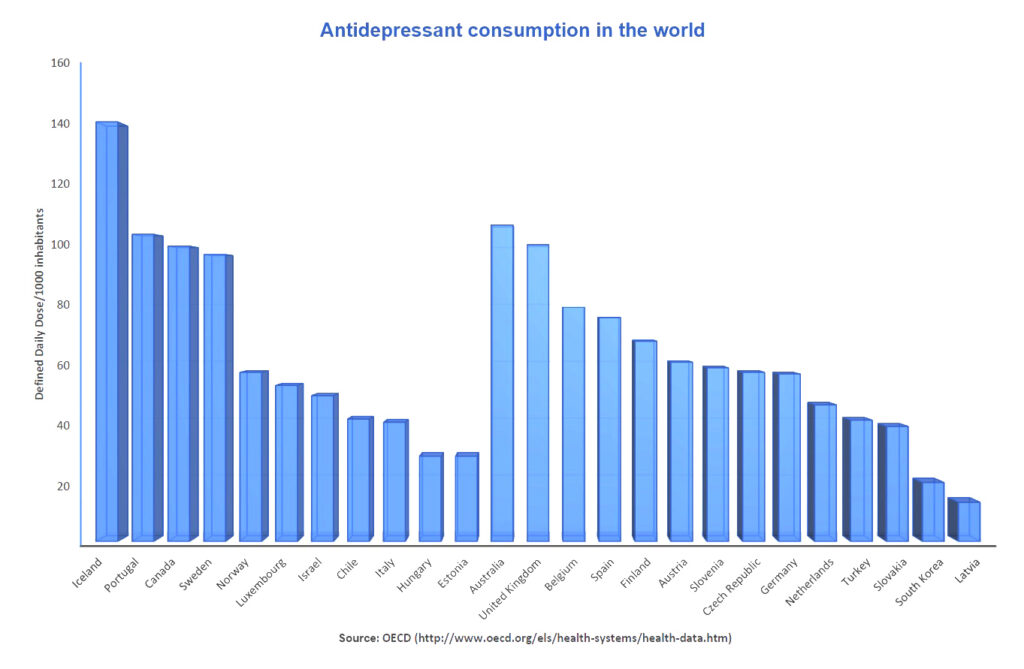
I believe that having the opportunity to know and observe (as operators, but not only) the daily experience of the carriers of a rare disease and their caregivers can be a continuous starting point for reflection and analysis of our era which, despite the extraordinary material well-being achieved, expresses great psychological distress, as evidenced by the data relating to the consumption of antidepressant drugs (Fig. 9) and psychoactive substances worldwide.