
2. WHY IS A DISEASE RARE?
Laura Mazzanti, Emanuela Scarano, Annamaria Perri
with the contribution of Federica Tamburrino, M.D., Ph.D.
Rare diseases now constitute a public health problem, due to their numerical impact on the population. In Italy, greater attention has been focused on rare diseases since the beginning of the 1990s. The Ministry of Health approved the National Rare Disease Plan 2013-2016 on October 16, 2014. Rarity leads to scarce availability of scientific knowledge and difficulties in obtaining an appropriate diagnosis, with long periods of latency between the onset of the disease, obtaining an appropriate diagnosis, and receiving adequate treatment, which often negatively affect the prognosis of the condition. If we then consider that some ultra-rare diseases affect individual family units, these diagnostic difficulties become even more evident.
Approximately 25% of the diseases affect pediatric patients (under 14 years of age), 28% in the Emilia-Romagna region. In children, the rare diseases that occur most frequently are congenital malformations (45%), in fact, congenital rare diseases with developmental defects represent a less numerous, but extremely important group from a clinical-diagnostic point of view. The annex to the Ministerial Decree 279/2001 listed 290 forms, however, following the new Decree of the President of the Council of Ministers (Prime Ministerial Decree) of 12 January 2017 and the related update of the Essential Assistance Levels (LEA), the number was increased to 350. We then have diseases of the endocrine glands, followed by diseases of the metabolism and the immune system (20%). This is an estimate which is significantly lower than the 50-60% of pediatric cases, calculated internationally. For adult patients, however, the highest frequencies concern diseases of the nervous system, diseases of the sense organs (29%), pathologies of the blood and hematopoietic organs (18%).
2.1. Rare disease patients
People with rare diseases, especially children, are exposed to the great suffering and challenges of growing up with a rare disease (condition), involving the whole family context: parents, siblings, and relatives. All children and their families live a twofold painful experience, characterized, on the one hand, by the pathological condition that requires frequent clinical visits, and sometimes even invasive procedures and, on the other hand, by a condition of loneliness, linked to the scarcity of available scientific knowledge. It is very difficult to accept a rare disease and it is essential to learn to live with it. Many rare diseases are complex, serious, degenerative, chronically disabling: about a third lower life expectancy to less than 5 years; many, however, do not significantly affect lifespan if they are diagnosed promptly and treated appropriately; others allow people to live a normal life, even without treatment.
2.2. Diagnosis and diagnostic difficulties
Rare diseases are characterized by their large number and by the numerous symptoms that vary not only from condition to condition, but also from patient to patient, even with the same disease. Due to their low prevalence and their specificity, diagnosing rare diseases requires experience in rare conditions and a good knowledge of normal variants. The inadequacy of scientific knowledge prevents patients, in the majority of cases, from obtaining effective treatments and care. Rare diseases very often affect various organs and have complex and often multi-systemic clinical pictures, which require the coordinated intervention of numerous specialists, thus a global multi-disciplinary approach, with very complex diagnostic and follow-up pathways (Douzgou et al. 2014; Vasudevan, Suri 2017); 40-50% of conditions still remain without a diagnosis today. On the basis of the foregoing, the importance of an early and precise diagnosis emerges in subjects with indicative or suggestive phenotypic aspects. Early diagnosis and an adequate follow-up to prevent any complications related to the syndromic condition are even more important when dealing with subjects of developmental age.
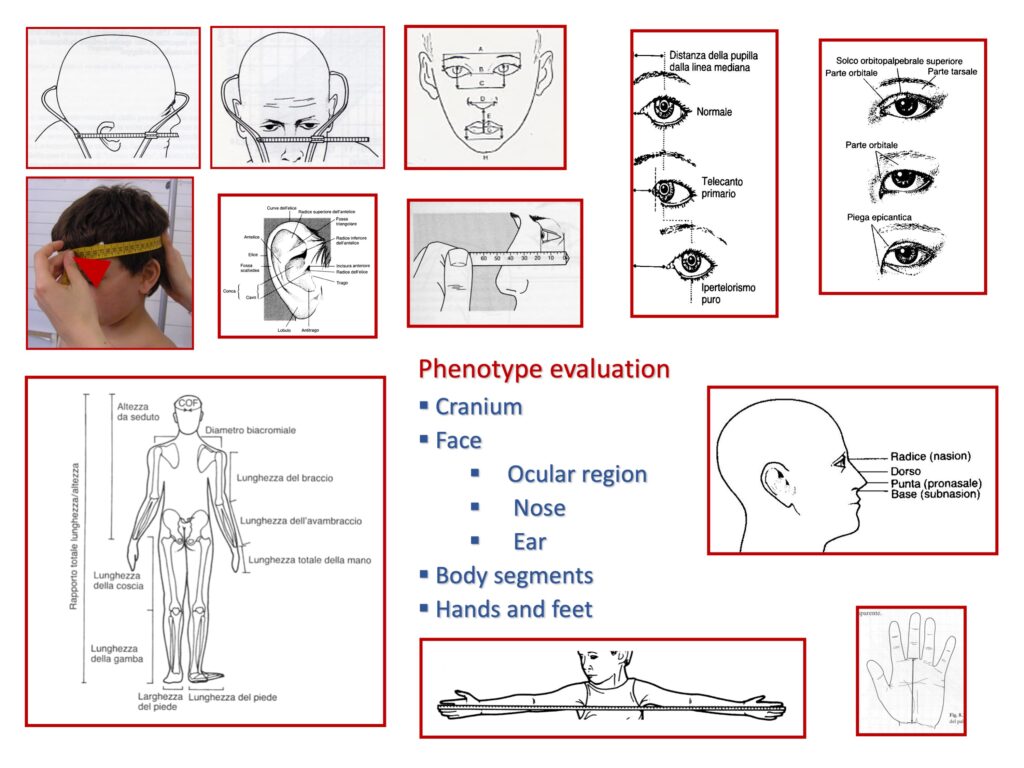
The diagnosis of rare diseases requires specific multidisciplinary skills aimed at recognizing, following and treating the various anomalies detected in the individual, and carrying out accurate family screening (Hall 1993). The analysis of the phenotype to detect major or minor anomalies is a science called Dysmorphology. It is primarily a visual specialty and the ability to be an accurate observer is obtained over time, by developing a sense of dimension, proportion, position, and symmetry (Fig. 2) (Hunter 2002).
We now have new diagnostic tools, such as Next-Generation Sequencing (NGS), which facilitate large-scale diagnosis, allowing for the evaluation of many genes in a single analysis (Hennekam, Biesecker 2012; Nambot, et al. 2018). On the other hand, even with the use of these powerful diagnostic methods, the evaluation of the phenotype and the genetic-clinical evaluation remain essential. Biology is very complex, the phenotypes of subjects with rare diseases are caused by a combination of the actions of multiple genes, epigenetic influences, and the environment. Here the essential role of physicians with expertise in rare diseases and clinical geneticists comes into play, as they must hone their diagnostic skills by switching from the pre-NGS-test to the post-NGS-test differential diagnosis modes (Robin 2018). In the era of genomic medicine, the integration of the hypotheses of experienced syndromologists and NGS techniques will be very productive in terms of translational research and clinical activity.
2.3. Expertise of medical personnel in the diagnosis of rare diseases
It is essential to have medical experts in the field of diagnostics with adequate training and who also carry out research. In fact, research, both clinical and basic, plays an important role and is recognized as an instrument of choice for increasing knowledge on rare diseases, contributing to the progress of medical research in general, while also having a huge impact on common diseases. In fact, rare diseases act both as an experimental model to increase knowledge on the physiology of growth and development processes, and as a “laboratory” for new health policies.
2.3.1. Continuing medical education
Training represents a crucial aspect in the field of rare diseases. The growth and professional assessment of healthcare workers is an essential requirement, which must be ensured through continuing medical education. Basic and specialist training is undertaken at the university level, through university courses and graduate school programs; professional updating is then organized at national and regional levels. Specific courses are offered in the degree courses in Medicine, in the training program of some specialization schools and in post-graduate degrees, yet it is desirable that this training be more common in programs, both basic and specialised, as stated by the Ministry of Health in the National Rare Disease Plan 2013-2016 (Ministry of Health 2014).
2.3.2. Networks for rare diseases
Rare diseases, due to their characteristics of multi-organ complexity and rarity, require the establishment of competent points of reference for both patients and general practitioners, and the specialists who do not have an in-depth knowledge of rare diseases. In the management of activities involving a high degree of specialization, such as rare diseases, specific and combined interventions are necessary in order to prevent morbidity and improve the quality of life of those affected. It goes without saying that interregional and international networks are therefore indispensable.
At the national level. In 2001 the Ministerial Decree n. 279 had listed the diseases and rare disease groups, each identified by a specific code, for which the right to exemption from participation in the cost for the related health care services, included in the LEA, was recognized, with the identification of accredited centers for the diagnosis and treatment of rare diseases by the Regions. As already specified, the recent Prime Ministerial Decree of January 2017 defined the new LEAs by extending the list of rare diseases.
The Emilia-Romagna Region has applied the Hub & Spoke network model, identifying highly specialized centers in the field of rare diseases, in which clinical cases and expertise are concentrated and connected by the network. Their collaboration leads to the definition of shared diagnostic-therapeutic pathways, in order to offer diagnostics and, subsequently, homogeneous healthcare to patients. Therefore, various networks have been set up dedicated to single pathologies or groups of pathologies (Emilia-Romagna Region, Regional Council Resolution of 19 September 2017, no. 1351).
At the international level. The need to offer people with rare diseases the most up to date knowledge and the most reliable information, in order to improve their medical assistance and quality of life, led the European Commission, in 2016, to launch a call for the development of European Reference Networks for Rare Diseases (ERN, European Reference Network) between member states. ERNs are networks of centers of expertise providing healthcare, with an organization that goes beyond the borders of the individual state. The collaboration between the member states of the European Union can, in fact, provide valuable support for sharing expertise, ensuring the exchange of knowledge between medical professionals. The Italian Ministry of Health joined the call and Italy was granted approval to participate in 23 of the 24 European Reference Networks, in which 63 hospitals and 187 units are involved, as full members.
In this regard, the centers of expertise for rare diseases or Health Care Providers (HCP) of the University of Bologna that received recognition as ERN were:
- the Rizzoli Orthopedic Institute of Bologna (included in BOND, the European Reference Network on Bone Disorders, and in EURACAN, the European Reference Network on congenital and hereditary anomalies);
- the S. Orsola University Hospital of Bologna (ENDO, the European Reference Network on endocrine conditions; EURACAN; ITHACA, the European Reference Network on congenital malformations and rare intellectual disabilities; LUNG, the European Reference Network on respiratory diseases; SKIN, the European Reference Network on skin disorders);
- IRCCS, Institute of Neurological Sciences (EIPCARE, the European Reference Network on epilepsy; EURACAN).
2.3.3. Organization of centers of expertise (HCP) for rare diseases
To guarantee patients an adequate diagnostic pathway and ongoing care, with a defined pathway for follow-up, the centers experienced in rare diseases have competent and dedicated staff, and are required to implement a multidisciplinary care network. The diagnostic and therapeutic protocols prepared for single diseases and/or groups of diseases must be adopted as uniformly as possible, both nationally and internationally. The transition phase of the patient from pediatric age to adulthood must also be managed, in order to ensure continuity of care.
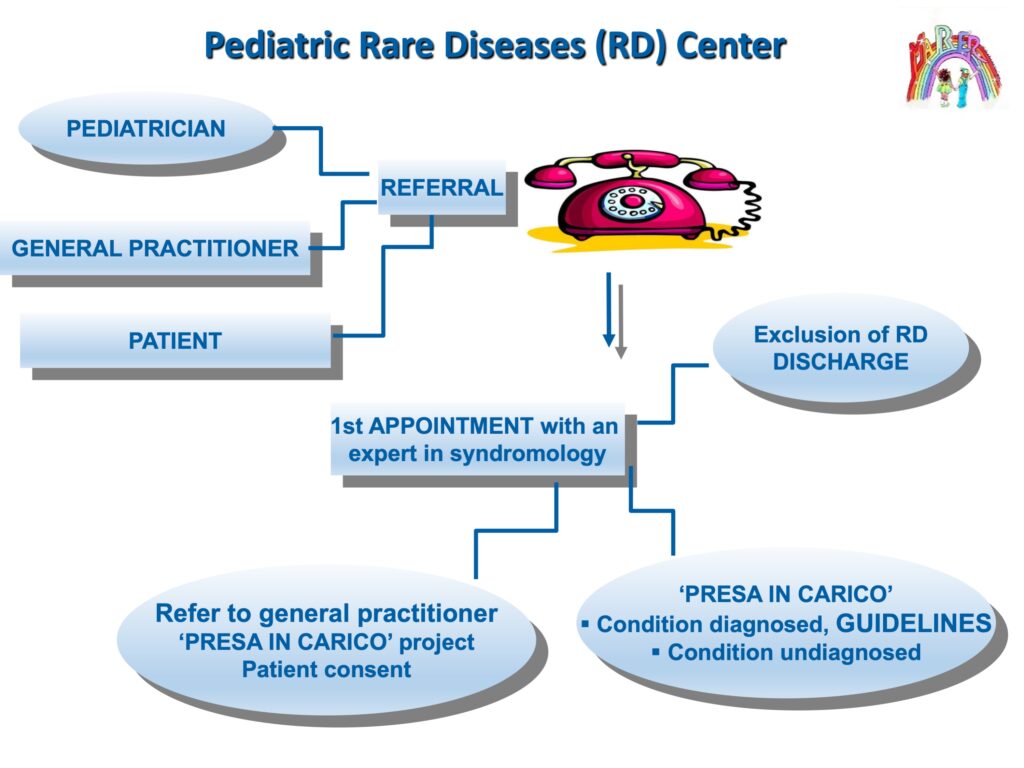
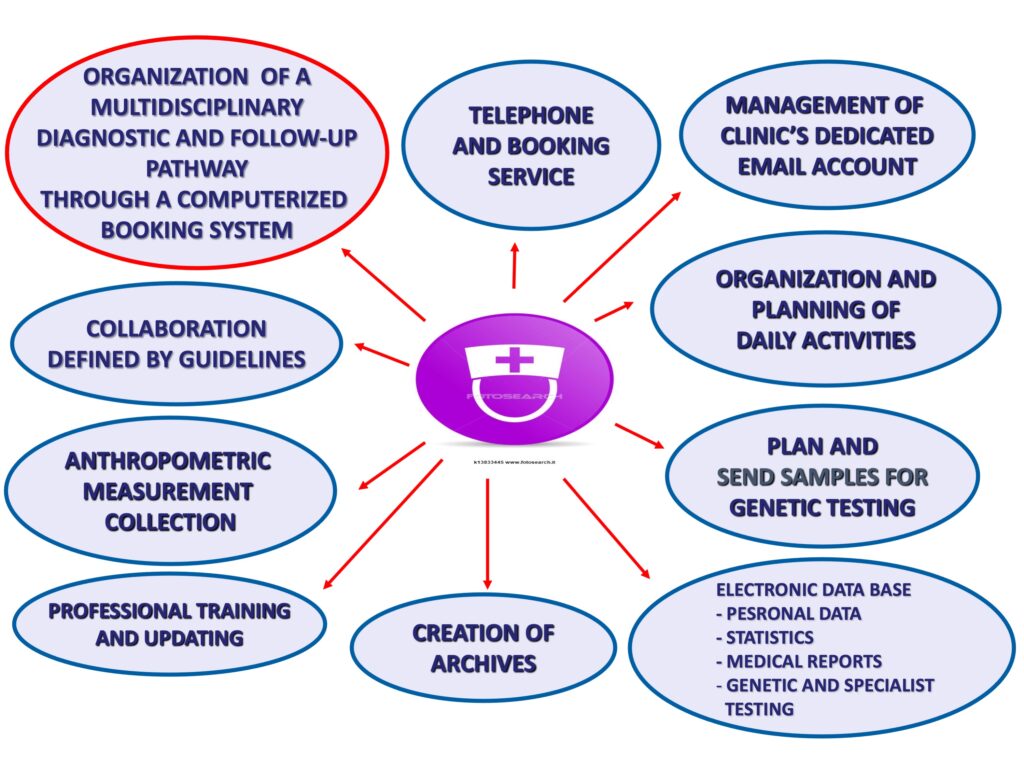
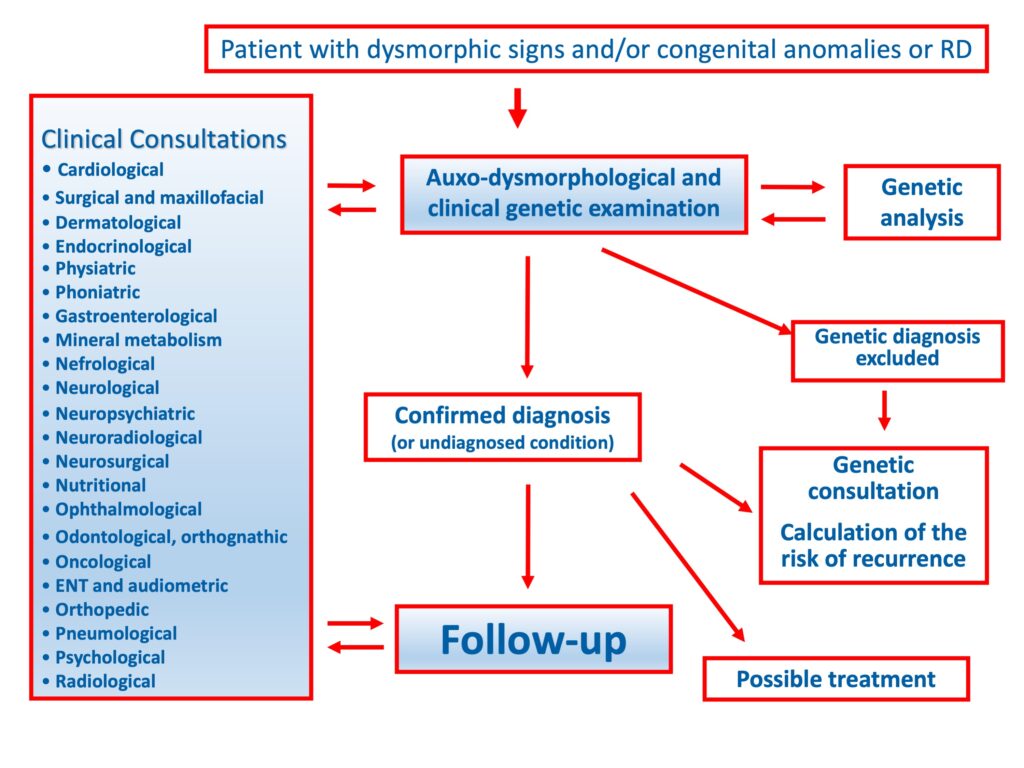
An example is the Pediatric Rare Diseases Center of Sant’Orsola, University Hospital in Bologna, Italy, which is recognized as a Regional Hub (Emilia-Romagna Region, Regional Council Resolution of 19 December 2011, n. 1897). The center has formalized a permanent multidisciplinary team of specialists, to share and optimize a network of multidisciplinary interventions, connected and coordinated for both the diagnosis and follow-up of patients, in order to manage the complex problems of subjects with rare diseases, creating an individualized clinical project (Figs. 3, 4, 5).
A clinic for undiagnosed rare diseases with developmental defects was also set up, in which experts in clinical syndromology, neonatologists, developmental pediatricians, clinical geneticists and any additional specialists from the multidisciplinary care network are present at the same time, to activate all the expertise of the hospital and apply the new molecular genetics technologies, in order identify ultra-rare conditions.
The multidisciplinary team includes the role of the clinical psychologist, as highly specialized psychological support is needed for these young patients and their families to promote a better quality of life, alleviate the burden on family and promote the social inclusion of children. The need for qualified psychological support is recognized in the international literature and in the most recent guidelines.
2.3.4. Volunteer associations
Volunteer associations are essential for centers that follow patients with rare diseases, since they bring the patient’s requests to the attention of the general population, in order to reduce their sense of loneliness, and can contribute to raising funds both for welfare purposes, where the public fail to cover needs, and to promote research.
2.4. Therapy and rare diseases
Successful etiological therapies are often lacking, but this does not imply that treating people with rare diseases is impossible. In fact, there are numerous symptomatic, supportive, rehabilitative, educational, replacement or supplementary functions, and palliative treatments, including some services currently not provided by the National Health Service, which can significantly change the clinical course and life expectancy, the degree of autonomy and quality of life of affected people and their families. Access to these already available treatments and their innovative aspects constitute key elements in the healthcare policies aimed at patients with rare diseases.